How to Read a Percent Gait Cycle Chart
Original Editor - Karsten De Koster Superlative Contributors -
Lucinda hampton,
Kim Jackson,
Nikhil Benhur Abburi,
Alexandra Kopelovich,
Admin,
Ayesha Arabi,
Maarten Cnudde,
Simisola Ajeyalemi,
Rucha Gadgil,
Tolulope Adeniji,
WikiSysopand
Vidya AcharyaIntroduction [edit | edit source]

Man gait depends on a circuitous interplay of major parts of the nervous, musculoskeletal and cardiorespiratory systems.
- The individual gait pattern is influenced past age, personality, mood and sociocultural factors.
- The preferred walking speed in older adults is a sensitive marker of full general health and survival.
- Condom walking requires intact cognition and executive control.
- Gait disorders lead to a loss of personal liberty, falls and injuries and consequence in a marked reduction in the quality of life[i].
Definitions [edit | edit source]
Gait - the manner or style of walking.
Gait Analysis -
An analysis of each component of the iii phases of ambulation is an essential part of the diagnosis of various neurologic disorders and the cess of patient progress during rehabilitation and recovery from the furnishings of neurologic affliction, a musculoskeletal injury or disease process, or amputation of a lower limb.
Gait speed
- The time it takes to walk a specified distance, usually vi m or less. Slower speeds correlate with an increased risk of bloodshed in geriatric patients.[2]
- Normal walking speed primarily involves the lower extremities, with the arms and trunk providing stability and balance.
- Faster speeds - body depends on the upper extremities and trunk for propulsion, balance and stability with the lower limb joints producing greater ranges of motility.[three]
The gait cycle is a repetitive blueprint involving steps and strides[iv]
A step is one unmarried pace
A pace is a whole gait bicycle.
Stride time - fourth dimension between heel strike of i leg and heel strike of the contralateral leg[4].
Step width - the mediolateral space between the two feet[4].
The demarcation betwixt walking and running occurs when
- periods of double support during the stance phase of the gait bicycle (both feet are simultaneously in contact with the ground) give way to two periods of double bladder at the beginning and the stop of the swing stage of gait (neither foot is touching the ground)[5].
The Gait Cycle [edit | edit source]

The sequences for walking that occur may be summarised as follows:[vi]
- Registration and activation of the gait command within the primal nervous system.
- Transmission of the gait systems to the peripheral nervous arrangement.
- Contraction of muscles.
- Generation of several forces.
- Regulation of joint forces and moments across synovial joints and skeletal segments.
- Generation of ground reaction forces.
The normal forrard step consists of two phases: stance stage; swing stage,
- The Stance stage occupies lx% of the gait cycle, during which one leg and foot are bearing most or all of the bodyweight
- The Swing phase occupies just 40% of it[4], during which the foot is not touching the walking surface and the bodyweight is borne past the other leg and foot.
- In a complete two-stride cycle both anxiety are in contact with the flooring at the aforementioned fourth dimension for near 25 per cent of the fourth dimension. This part of the cycle is called the double-support phase.Gait cycle phases: the stance stage and the swing phase and involves a combination of open and close chain activities.[3]
The 90 2d video beneath gives the basics of this cycle
[7]
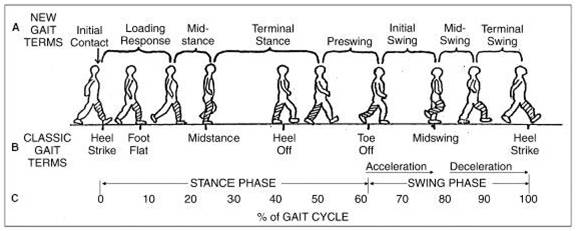
Phases of the Gait Bicycle (8 phase model): [4] [8]
- Initial Contact
- Loading Response
- Midstance
- Terminal Stance
- Pre swing
- Initial Swing
- Mid Swing
- Tardily Swing.[9]
Heel Strike (or initial contact) - Short period, begins the moment the foot touches the basis and is the first stage of double support.[three]
Involves:
- thirty° flexion of the hip: full extension in the articulatio genus: talocrural joint moves from dorsiflexion to a neutral (supinated 5°) position and then into plantar flexion.[iii] [4]
- Afterward this, genu flexion (5°) begins and increases, but equally the plantar flexion of the heel increased.[iv]
- Plantar flexion is allowed by eccentric contraction of the tibialis anterior
- Extension of the knee is caused past a wrinkle of the quadriceps
- Flexion is caused by a wrinkle of the hamstrings,
- Flexion of the hip is caused by the contraction of the rectus femoris.[4]
Foot Flat (or loading response phase)
- Body absorbs the touch on of the human foot by rolling in pronation.[3]
- Hip moves slowly into extension, caused by a contraction of the adductor magnus and gluteus maximus muscles.
- Knee flexes to 15° to 20° of flexion. [4]
- Talocrural joint plantarflexion increases to 10-fifteen°.[3] [4]
Midstance
- Hip moves from x° of flexion to extension past wrinkle of the gluteus medius muscle.[4]
- Human knee reaches maximal flexion and then begins to extend.
- Ankle becomes supinated[3] and dorsiflexed (five°), which is caused by some contraction of the triceps surae muscles.[3]
- During this phase, the body is supported by one single leg.
- At this moment the body begins to move from force absorption at impact to force propulsion forward.[3]
Heel Off
- Begins when the heel leaves the flooring.
- Bodyweight is divided over the metatarsal heads.[3]
- ten-13° of hip hyperextension, which so goes into flexion.
- Knee becomes flexed (0-5°)[iv]
- Ankle supinates and plantar flexes.[4]
Toe Off/pre-swing
- Hip becomes less extended.
- Knee is flexed 35-40°
- Plantar flexion of the ankle increases to 20°.[3] [4]
- The toes get out the basis.[4]
Early Swing
- Hip extends to 10° and and so flexes due to contraction of the iliopsoas muscle[iv] 20° with lateral rotation.[iii] [iv]
- Articulatio genus flexes to 40-threescore°
- Ankle goes from 20° of plantar flexion to dorsiflexion, to end in a neutral position.[3]
Mid Swing
- Hip flexes to 30° (by wrinkle of the adductors) and the ankle becomes dorsiflexed due to a contraction of the tibialis anterior musculus.[4]
- Knee flexes sixty° merely and so extends approximately xxx° due to the wrinkle of the sartorius musculus.[3] [4](caused by the quadriceps muscles).[3] [4]
Late Swing/declaration
- Hip flexion of 25-30°
- Locked extension of the human knee
- Neutral position of the ankle.[3]
Range of Motility during Gait
[x]
Ground Reaction Force during Gait
[11]
Muscular Activity during Gait
[12]
Gait Cycle - Anatomical Considerations [edit | edit source]
- Pelvic region - anterior-posterior deportation, which alternates from left to right. Facilitates anterior movement of the leg (each side anterior-posterior displacement of 4-5°).[three] [4] [eight]
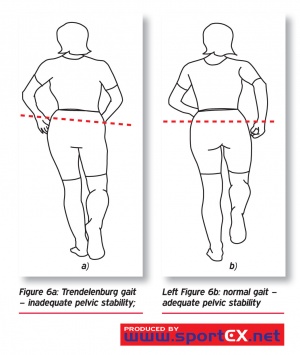
- Frontal plane - varus movement in the: foot between heel-strike and pes-flat and betwixt heel-off and toe-off; hip, in lateral movements (when the abductors are also weak, a Trendelenburg gait can be observed).[3] [8] Valgus movement betwixt pes-flat and heel off in the feet.
- A disorder in any segment of the trunk can have consequences on the individual's gait blueprint.[13]
Gait Disorders [edit | edit source]
Gait disorders - contradistinct gait pattern due to deformities, weakness or other impairments eg loss of motor control or hurting[14].

Prevelence increases with historic period and the number of people affected will essentially increase in the coming decades due to the expected demographic changes.
- Lead to a loss of personal freedom and to reduced quality of life.
- Precursors of falls and therefore of potentially severe injuries in elderly persons[ane].
Causes of gait disorders include
- Neurological, orthopedic, medical and psychiatric weather and multifactorial etiology becomes more than common with advancing age, making classification and management more complex.
- Whatever gait disorder should be thoroughly investigated in order to ameliorate patient mobility and independence, to prevent falls and to detect the underlying causes as early on as possible.
- Thorough clinical observation of gait, careful history taking focussed on gait and falls and physical, neurological and orthopedic examinations are bones steps in the categorization of gait disorders and serve as a guide for ancillary investigations and therapeutic interventions.
Gait Descriptions [edit | edit source]
This is not an exhaustive listing.
- Antalgic gait a limp adopted and then as to avoid pain on weight-begetting structures, characterized past a very short opinion phase.
- Ataxic gait an unsteady, uncoordinated walk, with a wide base and the anxiety thrown out, coming downward starting time on the heel and then on the toes with a double tap.This gait is associated with cerebellar disturbances and can exist seen in patients with longstanding alcohol dependency. People with 'Sensory'Disturbances may present with a sensory ataxic gait. Presentation is a broad base of operations of support, high steps, and slapping of anxiety on the floor in club to gain some sensory feedback. They may also need to rely on observation of human foot placement and will often look at the flooring during mobility due to a lack of proprioception
- Equine gait a walk accomplished mainly by flexing the hip joint; seen in crossed leg palsy.
- Parkinsonian Gait (seen in parkinson'south illness and other neurologic weather that affect the basal ganglia). Rigidity of joints results in reduced arm swing for balance. A stooped posture and flexed knees are a common presentation. Bradykinesia causes small steps that are shuffling in presentation. At that place may be occurrences of freezing or short rapid bursts of steps known as 'festination' and turning tin be difficult.
- Trendelenburg gait, the gait characteristic of paralysis of the gluteus medius musculus, marked by a list of the torso toward the afflicted side at each step.
- Hemiplegic gait a gait involving flexion of the hip because of footdrop and circumduction of the leg.
- Steppage gait the gait in footdrop in which the advancing leg is lifted high in order that the toes may articulate the ground. Information technology is due to paralysis of the anterior tibial and fibular muscles, and is seen in lesions of the lower motor neuron, such as multiple neuritis, lesions of the inductive motor horn cells, and lesions of the cauda equina.
- Stuttering gait a walking disorder characterized by hesitancy that resembles stuttering; seen in some hysterical or schizophrenic patients likewise as in patients with neurologic harm.
- Tabetic gait an ataxic gait in which the feet slap the ground; in daylight the patient can avoid some unsteadiness by watching his anxiety.
- Waddling gait exaggerated alternation of lateral body movements with an exaggerated summit of the hip, suggesting the gait of a duck; characteristic of muscular dystrophy.
- Diplegic Gait (Spastic gait). Spasticity is normally associated with both lower limbs. Contractures of the adductor muscles tin create a 'scissor' type gait with a narrowed base of support. Spasticity in the lower half of the legs results in plantarflexed ankles presenting in 'tiptoe' walking and frequently toe dragging. Excessive hip and knee joint flexion is required to overcome this
- Neuropathic Gaits. High stepping gait to gain floor clearance often due to foot driblet[thirteen] [14] [15] [2]
Musculoskeletal Causes:
Pathological gait patterns resulting from musculoskeletal are often caused by soft tissue imbalance, joint alignment or bony abnormalities affect the gait pattern every bit a issue[fourteen].
Hip Pathology
- Arthritis is a common cause of pathological gait. An arthritic hip has reduced range of movement during swing stage which causes an exaggeration of movement in the opposite limb 'hip hiking[14].
- Excessive Hip Flexion tin can significantly alter gait pattern near commonly due to; • Hip flexion contractures • It band contractures, • Hip flexor spasticity, • Compensation for excessive knee flexion and talocrural joint DF, • Hip pain • Bounty for excess ankle plantar flexion in mid swing. The deviation of stance phase will occur mainly on the affected side. The result is forward tilt of the trunk and increased demand on the hip extensors or increased lordosis of the spine with anterior pelvic tilt. A person with reduced spinal mobility will adopt a forward flexion position in club to alter their centre of gravity permanently during gait.
- Hip Abductor Weakness. The abductor muscles stabilise the pelvis to allow the opposite leg to elevator during the swing stage. Weak abductor muscles will cause the hip to drop towards the side of the leg swinging forward. This is also known every bit Trendelenburg gait[15]
- Hip Adductor Contracture. During swing stage the leg crosses midline due to the weak adductor muscles, this is known equally 'scissor gait'[fifteen]
- Weak Hip Extensors will cause a person to accept a smaller step to lessen the hip flexion required for initial contact, resulting in a lesser forcefulness of contraction required from the extensors. Overall gait will be slower to allow time for limb stabilisation. Compensation is increased posterior trunk positioning to maintain alignment of the pelvis in relation to the torso[15]
- Hip Flexor Weakness results in a smaller stride length due to the weakness of the musculus to create the forward move. Gait volition likely be slower and may result in decreased floor clearance of the toes and create a drag
- Knee joint Pathologies
- Weak Quadriceps. The quadriceps role is to eccentrically command the knee joint during flexion through the stance stage. If these muscles are weak the hip extensors volition compensate by bringing the limb back into a more extended position, reducing the amount of flexion at the knee during stance stage. Alternatively heel strike volition occur before increasing the ankle of plantar flexion at the ankle, preventing the forward movement of the tibia, to help stabilise the knee joint[15].
- Astringent Quadriceps Weakness or instability at the human knee joint will present in hyperextension during the initial contact to stance stage. The articulatio genus volition 'snap' back into hyperextension every bit the bodyweight moves forwards over the limb[fifteen]
- Genu Flexion Contraction volition cause a limping blazon gait design. The knee joint is restricted in extension, meaning heel strike is limited and step length reduced. To compensate the person is probable to 'toe walk' during opinion phase. Knee flexion contractures of more than thirty degrees will be obvious during normal paced gait. Contractures less then this will be more axiomatic with increased speeds[14] [15].
Talocrural joint Pathologies
- Ankle Dorsiflexion Weakness results in a lack of heel strike and decreased floor clearance. This leads to an increased pace height and prolonged swing phase[15].
- Calf Tightening or Contractures due to a period of immobilisation or trauma will crusade reduced heel strike due to restricted dorsiflexion. The compensated gait result volition be 'toe walking' on stance stage, reduced step length, and excessive knee and hip flexion during swing phase to ensure floor clearance[fourteen].
Footathologies
- Hallux Rigidus results in a lack of dorsiflexion of the corking toe. The MPJ uses the windlass effect to raise the curvation and stiffen the foot during dorsiflexion of the hallux. This stiffness increases the efficiency of the propulsion portion of the gait cycle. To be efficient in creating stiffness, the hallux should exist able to dorsiflex at least 65 degrees.
Leg length discrepancy
- Leg length discrepancy can exist as a result of an asymmetrical pelvic, tibia, or femur length or for other reasons such as scoliosis or contractures. The gait pattern volition present every bit a pelvic dip to the shortened side during the opinion phase with possible 'toe walking' on that limb. The opposite leg is likely to increase its knee and hip flexion to reduce its length[fourteen].
Antalgic Gait
- Antalgic gait due to human knee pain presents with decreased weight bearing on the affected side. The human knee remains in flexion and possible toe weight-bearing occurs during stance phase[fourteen]
- Antalgic gait due to ankle pain may present with a reduced step length and decreased weight bearing on the affected limb. If the trouble is pain in the forefoot so toe-off will be avoided and heel weight-bearing used. If the pain is more in the heel, toe weight-bearing is more likely. General ankle hurting may event in weight-bearing on the lateral edge[14] [15].
- Antalgic gait due to hip pain results in a reduced stance phase on that side. The body is propelled speedily forwards with the opposite shoulder lifted in an attempt to even the weight distribution over the limb and reduce weight-bearing. Swing phase is as well reduced[xiv].
Summary of Gait Deviations
| Observed Gait Departure | Likely Impairement | Compensation/Mechanical Rationale |
| Hip | ||
| Backward leaning of the torso during loading phase | Weak Hip Extensors | The line of gravity of the body moves behind the hips thereby reducing the need for hip extension torque |
| Frontward bending of the trunk during loading response | Weak Quadriceps | The torso is moved forward to bring the line of gravity inductive to the axis of rotation of the human knee and reducing the need for knee extensors |
| Lateral torso lean towards the stance (Compensated Trendelenburg Gait) | Marked weakness of the hip abductors Hip pain | Shifting of the trunk over the unaffected lower extremity reduces the need of the hip abductors |
| Hip Circumduction (semicircle movement of the hip during swing stage) | Hip flexor weakness | Semicircle movement includes the combination movement of hip flexion, hip abduction and forward rotation of the pelvis |
| Knee | ||
| Flexed position of the genu during stance despite normal range of motion at the genu joint | Impairement at the talocrural joint or the hip joint (Bounty occurring at the knee articulation) | Exaggerated hip flexion or ankle dorsiflexion during stance results in flexion of the human knee |
| Excessive articulatio genus flexion during swing phase | Reduced talocrural joint dorsiflexion of the swing limb | Increment toe clearance of the swing limb. (This is accompanied with increased hip flexion) |
| Knee is kept in extension during loading phase (No extension thrust is observed) | Weak quadriceps | Anterior trunk lean is observed during early stance, thereby moving the line of gravity of the trunk slightly inductive to the centrality of rotation |
| Reduced knee flexion during swing phase | Knee extension contracture | Hip hiking or hip circumduction will exist observed as bounty |
| Ankle | ||
| Foot slap Quick ankle plantar flexion occurring later on heel contact | Weakness in ankle dorsiflexors | None/less active dorsiflexion occurs during swing phase Normal dorsiflexion tin can occur during opinion phase (if there is normal range of motion at the talocrural joint joint) |
| Drop Foot Ankle remains in plantar flexion during swing stage | Weakness in ankle dorsiflexors | To prevent toes from dragging during the swing phase hip circumduction, hip hiking or exaggerated hip and knee flexion volition be noted |
[sixteen]
Below are links to videos demonstrating normal gait and various gait abnormalities:
| [17] | [18] |
| | |
Age-Related Gait Changes
Ageing is marked with cerebral decline, reduction in joint motion due to osteopenia and osteoporosis.[19] And most peculiarly plantar flexors loss that reduce stance phase in this population with reduction in vigil for auditory, vestibular, visual and somatosensory system.[20] [21] This factors interplay to results in increase in prevalence of gait disorders among older adults.
As well, whatever threat to balance induces changes in the strategies for continuing and walking - the opinion and gait base is widened, bipedal floor contact is prolonged, step length becomes shorter, the feet are lifted less loftier during the swing phase, walking becomes slower and the posture becomes stooped.

- The fear of falling and the actual hazard of falling increment with age.
- Older persons are therefore more probable to use these protective gait strategies.
- As muscle power diminishes and proprioception and vision become impaired with age,
- body sway on standing, which is constantly nowadays to a slight degree, increases.
- In younger persons this sway can be compensated by activating the muscle groups around the upper ankle joints. Older persons shift this bounty to the proximal muscle groups around the hips due to loss of distal proprioception.
- This requires an increased reliance on vestibular afferent, which undergo less modify during the ageing procedure.
- The preferred walking speed in patently good for you elderly subjects declines by one % per year from a mean of 1.three grand/s in the seventh decade to a mean of 0.95 thou/southward in those anile over 80 years (caused by a decrease in step length rather than past a change in cadency).
- Gait changes are to some degree a consequence of normal ageing however individual walking speed in elderly subjects is a stiff indicator of full general health and survival[1]
Some specific changes observed in elements of gait every bit affected in older adults are not limited to:
- reduction in gait velocity (speed of walking) due to shorter steps but at the aforementioned rate (cadence).
- And increase in time spent in double stance phase
Because of multi-decline in body physiological functions and prevalent of multi-morbidity amidst this population it is non uncommon to have mixtures of neurological and musculoskeletal related gait disorders in this population.[22] Common gait disorders in older adults under neurological causes are sensory ataxia, Parkinsonism & frontal gait disorders. While non-neurological ( includes hip and knee osteoarthritis.[23]
Gait Analysis [edit | edit source]
- The analysis of the gait wheel is important in the biomechanical mobility exam to proceeds information near lower limb dysfunction in dynamic motion and loading.[24]
- When analyzing the gait cycle, it is all-time to examine one joint at a time.[3]
- Objective and subjective methods tin can be used.[25] [26]
Subjective
- Dissimilar gait patterns - We might ask the individual to walk normally, on insides and outsides of feet, in a straight line, running (all the fourth dimension looking to compare sides and understanding of "normal").
- Inquire/find the type of footwear the patient uses (a systematic review suggests shoes affect velocity, pace fourth dimension, and pace length in younger children's gait[27]).
Objective
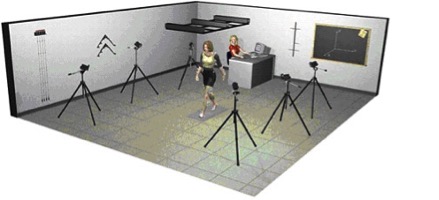
An objective arroyo is quantitative and parameters like time, distance, and muscle activeness will be measured. Other objective methods to appraise the gait cycle that use equipment include:[28] [26]
- Video Analysis and Treadmill
- Electronic and Computerized Apparatus
- Electronic Pedometers
- Satellite Positioning Organisation[25]
Qualitative methods to assess and analyse gait include: [26]
- Rancho Los Amigos Hospital Rating List[29]
- Ten Meter Walking Test[30]
- vi Infinitesimal Walk Test
- ii Minute Walk Exam
- Dynamic Gait Index
- Emory Functional Airing Contour[31]
- Timed Up and Get Test[32] This test is statistically associated with falling in men, but not in women.
- Functional Ambulation Categories[33]
- Tinetti-Test[34]
Clinical Bottom Line [edit | edit source]
Good knowledge of beefcake and biomechanics is important to understand the different phases of the gait cycle. When you know the normal pattern, y'all tin can see what'due south going wrong!
References [edit | edit source]
- ↑ i.0 i.i 1.two Pirker W, Katzenschlager R. Gait disorders in adults and the elderly. Wiener Klinische Wochenschrift. 2017 Feb i;129(iii-four):81-95.Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5318488/ (final accessed 27.half dozen.2020)
- ↑ 2.0 ii.1 Medical dictionary Gait speed Available from: https://medical-dictionary.thefreedictionary.com/gait+speed (concluding accessed 28.6.2020)
- ↑ 3.00 3.01 three.02 3.03 iii.04 3.05 3.06 3.07 3.08 3.09 3.ten 3.11 3.12 3.13 3.14 3.15 3.16 three.17 three.xviii Shultz SJ et al. Examination of musculoskeletal injuries. 2nd ed, North Carolina: Man Kinetics, 2005. p55-60.
- ↑ 4.00 4.01 4.02 iv.03 iv.04 4.05 four.06 4.07 4.08 4.09 4.10 4.11 four.12 4.13 iv.14 4.15 4.16 4.17 4.18 4.xix 4.20 Loudon J, et al. The clinical orthopedic assessment guide. 2d ed. Kansas: Human Kinetics, 2008. p.395-408.
- ↑ The biomechanics of running Tom F. Novacheck Motion Analysis Laboratory, Gillette Children's Specialty Healthcare, Uni6ersity of Minnesota, 200 E. Uni6ersity A6e., St. Paul, MN 55101, USA Received 25 August 1997; accepted 22 September 1997 Available from:
- ↑ Vaughan CL. Theories of bipedal walking: an odyssey. J Biomech 2001;36(2003):513-523.Available fromhttp://citeseerx.ist.psu.edu/viewdoc/download?doi=x.1.1.468.2414&rep=rep1&type=pdf
- ↑ Nicole Comninellis The Gait Bike Blitheness Available from https://www.youtube.com/sentinel?time_continue=35&5=DP5-um6SvQI
- ↑ 8.0 8.1 viii.2 Demos, Gait analysis, (http://world wide web.ncbi.nlm.nih.gov/books/NBK27235/), 2004.
- ↑ Berger W, et al. Cosmetic reactions to stumbling in man: neuronal co-ordination of bilateral leg activity during gait. J Physiol 1984;357: 109-125.
- ↑ Alexandra Kopelovich. Gait Range of Move Available from: https://www.youtube.com/watch?v=5Z6shSu96CM [last accessed 31/iii/2021]
- ↑ Alexandra Kopelovich. Ground Reaction Force During the Gait Cycle Available from: https://www.youtube.com/watch?v=Y2RHvicAM2o [last accessed 31/3/2021]
- ↑ Alexandra Kopelovich. Gait Muscular Activity & Activity. Available from: https://world wide web.youtube.com/watch?5=WuG87mRiY-8[last accessed 31/iii/2021]
- ↑ 13.0 13.1 Shi D, et al. Consequence of anterior cruciate ligament reconstruction on biomechanical features of knee joint level in walking: a meta assay. Chin Med J 2010;123(21):[[1]].
- ↑ 14.0 xiv.1 14.2 14.three xiv.4 14.5 14.half dozen 14.7 fourteen.8 fourteen.9 Malanga M and Delisa J.A. Department Ane: Clinical Ascertainment. Part of rehabilitation Enquiry and Development No Date. http://world wide web.rehab.inquiry.va.gov/mono/gait/malanga.pdf (accessed 6 February 2010)
- ↑ xv.0 15.1 fifteen.2 15.iii 15.4 fifteen.5 fifteen.6 15.7 fifteen.eight University of Washington. Pathologic Gait: Musculoskeletal http://courses.washington.edu/anatomy/KinesiologySyllabus/PathGait1Ortho.pdf (accessed five February 2015)
- ↑ ane. Neumann, D.A. Kinesiology of the Musculoskeletal System. (3 ed.). : Elsevier; 2017
- ↑ onlinemedicalvideoAbnormal Gait Exam : Myopathic Gait Demonstration. Available fromhttps://www.youtube.com/watch?time_continue=v&five=b5rIEx9SsCo
- ↑ scfpta gait deviation published final 001.wmvAvailable fromhttps://world wide web.youtube.com/sentry?time_continue=v&v=b5rIEx9SsCo
- ↑ Pirker W, Katzenschlager R. Gait disorders in adults and the elderly. Wiener Klinische Wochenschrift. 2017 Feb;129(3):81-95.
- ↑ Tzu-wei PH, Shorter KA, Adamczyk PG, Kuo AD. Mechanical and energetic consequences of reduced ankle plantar-flexion in human walking. Journal of Experimental Biology. 2015 Nov 1;218(22):3541-l.
- ↑ Panizzolo FA, Dark-green DJ, Lloyd DG, Maiorana AJ, Rubenson J. Soleus fascicle length changes are conserved betwixt young and quondam adults at their preferred walking speed. Gait & posture. 2013 Sep 1;38(4):764-nine.
- ↑ Pirker W, Katzenschlager R. Gait disorders in adults and the elderly. Wiener Klinische Wochenschrift. 2017 February;129(3):81-95.
- ↑ Pirker W, Katzenschlager R. Gait disorders in adults and the elderly. Wiener Klinische Wochenschrift. 2017 Feb;129(3):81-95.
- ↑ Langer PS, et al. A applied manual of clinical electrodynography. 2nd ed. Deer Park: The Langer Foundation for Biomechanics and Sports Medicine Research, 1989.
- ↑ 25.0 25.1 Terrier P, Schutz Y. How useful is satellite positioning system (GPS) to rails gait parameters? A review. J Neuro Eng Rehab 2005;2:28.
- ↑ 26.0 26.1 26.2 Deckers JHM, et al. Ganganalyse en looptraining voor de paramedicus, Houten, Bohnfleu van Lonhum, 1996.
- ↑ Cranage S, Perraton 50, Bowles KA, Williams C. The impact of shoe flexibility on gait, force per unit area and musculus action of young children. A systematic review. Journal of Foot and Ankle Inquiry. 2019 Dec 1;12(1):55.
- ↑ Frigo C, et al. Functionally oriented and clinically feasible quantitative gait analysis method. Med Biol Eng Comput 1998;36:179-185.
- ↑ Shumway-Cook A, Woollacott MH. Motor control: translating research into clinical practice. Lippincott Williams and Wilkins, 2007. p.408.
- ↑ Van Peppen RPS, KNGF-richtlijn Beroerte, 2004, Nederlands Tijdschrift voor Fysiotherapie.
- ↑ Baer RH, Wolf SL. Modified emory functional ambulation contour: an outcome mensurate for the rehabilitation of post stroke gait dysfunction. Stroke 2001;32(four):973-979.
- ↑ Potsiadlo D, Richardson S. The timed "Up and Go": a test of functional mobility for frail elderly persons. J Am Geriatr Soc 1991;39(2):142-148.
- ↑ Shephard RJ, Taunton JE. Foot and ankle in sport and exercise, Toronto:Karger, 1987. p30-38.
- ↑ Bautmans I, et al. The feasibility of whole trunk vibration in institutionalised elderly persons and its influence on muscle performance, rest and mobility: a randomised controlled trial. BMC Geriatr 2005;v:17.
Source: https://www.physio-pedia.com/Gait
0 Response to "How to Read a Percent Gait Cycle Chart"
Enregistrer un commentaire